- Technical Advances Article
- Open access
- Published:
Cone-wedge anchored surgical templates for stackable metal guide: a novel technique
International Journal of Implant Dentistry volume 10, Article number: 27 (2024)
Abstract
Objective
To address the instability in implant surgical guides, this technique proposes an alternative anchoring mechanism in the stackable metal surgical guides utilizing cone-wedge anchors for improved stability.
Methods
Postoperative implant position superimposed onto the preoperatively planned design using Mimics Medical 21.0 and Materialise Magics 24.0 to assess 3D coronal implant deviation, 3D apical implant deviation, and implant angular deviation.
Results
Postoperative cone-beam computed tomography (CBCT) revealed a high level of precision in the implant placement, with an average 0.97 mm deviation at implant coronal region, 1.56 mm at implant apexes, and 2.95° angular deviation.
Conclusion
This technique introduces a novel cone-wedge anchoring mechanism to enhance the stability of stackable metal surgical guide templates, addressing inherent instability issues. The utilization of this approach significantly improves the accuracy of implant placement procedures.
Introduction
Computer-assisted implant surgery (CAIS) is considered optimal for placing dental implants in the desired prosthetic and anatomical position [1, 2]. Owing to cone-beam computed tomography (CBCT) scanning [3], virtual planning software [4], computer-aided manufacturing technology (CAM) [5], and other digital technology development, virtual implant plans can be realized in clinical settings. Static surgical guides are vital mediums for transferring the preoperative virtually designed implant position into the patient’s mouth. Although surgical guides can significantly increase the precision of implant surgery, there is still an inevitable deviation between the preoperative design and postoperative position. The errors mainly originate from imaging collection [4], data transfers [6], template manufacturing [7], surgical template positioning [8], operator’s experience [9], drill macro-design [10], and drilling strategy (sleeve height, drilling distance, drilling key length) [11].
Surgical template fixation and stabilization during the implant bed preparation may have caused the high deviation in the final implant position [12]. Sequential implant surgical templates are typically utilized for full-arch edentulous patients, which are made up of several subset templates to function in scenarios such as template retention, bone reduction, or implant placement. These subset templates share the same retainer pins anchored on the alveolar bone. However, once the bone retainer pins are removed, the repositioning of the pins may be difficult. Therefore, a stackable surgical template was proposed [13]. Typically, a stackable surgical template possesses two parts: the base template and the super-structure templates. The base template is connected to the alveolar bone by retainer pins, and the super-structural templates need to connect to the base template. According to its function in surgery, the super-structural templates can be categorized into several subset templates such as positioning template, bone reduction template, and implant template. A stackable surgical template takes the strategy that the base template is precisely fixed on the alveolar bone by bone retainer pins with the help of the positioning template, and the upper-structure templates (such as the positioning template, the bone reduction template, and implant placement template) are anchored to the base template via different fixation approaches, correspondingly. For improved accuracy, some studies have focused on the fixation modification between the base template and the upper-structure templates, such as bead-anchored structure [8], magnetically retained structure [14,15,16], strut-based lattice structure [13], ball-snap structure [17], and pin-anchored structure [18].
This study proposes a novel cone-wedge anchorage technique to connect and stabilize the upper-structure templates to the base template and to improve surgical template fixation and stabilization.
Technique
-
1.
Extract the remaining teeth and fabricate a diagnostic denture after 3 months when the hard and soft tissue recovered (Fig. 1A, B). Attach the smile line and fiducial to the dentures which served as radiographic templates for CBCT scanning (Newtom VGi) using the dual scan technique (Fig. 1C, D, E) [19, 20].
Fig. 1 
A, Preoperative intraoral photograph of maxillary. B, Preoperative intraoral photograph of mandibular. C, Radiographic examination. D, Maxillary diagnosis denture with smile line. E, Mandibular diagnosis denture
-
2.
Import the Digital Imaging and Communications (DICOM) files into a computer-aided design (CAD) surgical implant planning program (3Shape 2020), and perform prosthetically driven computer-aided implant planning. Plan four dental implants with four fixation pins in the maxillary and two implants with three fixation pins in the mandible (Template Fixation Pin 1.5 × 32 mm, Inclusive). Import the surgical implant guide information using standard tessellation language (STL) files into the forward engineering software (Materialise 3-matic 20.0) and design the metallic retainer template and implant placement templates (Fig. 2A-D).
Fig. 2 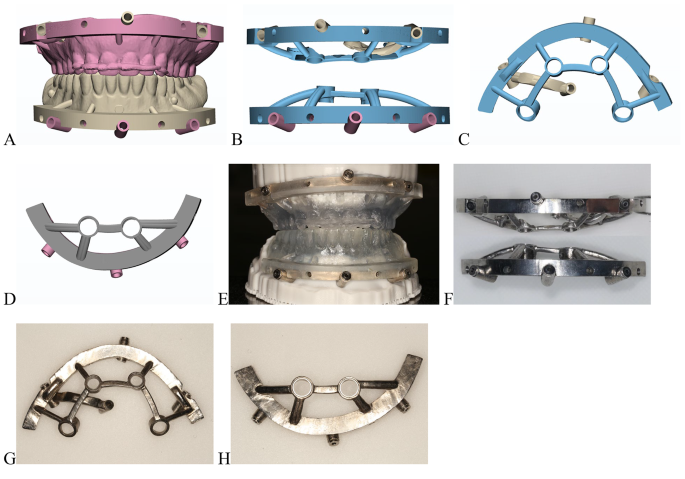
Digital designs and metal surgical templates. A and E, 3D-printed positioning temporary teeth. B and F, Cone-anchored metal stackable template in a horizontal direction. C and G, Maxillary template. D and H, Mandibular template
-
3.
Manufacture the titanium alloy surgical templates with three-dimensional (3D) printing technology of selective laser melting (SLM) (Chamlion NCL-M2150T, China) (Fig. 2E-H). Design the cone-wedges and temporary teeth for assisted positioning (Materialise Magics 21.0), and 3D-print them using photosensitive resin (Heygears Surgical Guide UV resins, with Heygears Streamflow Dental 3D Printer) (Fig. 3).
Fig. 3 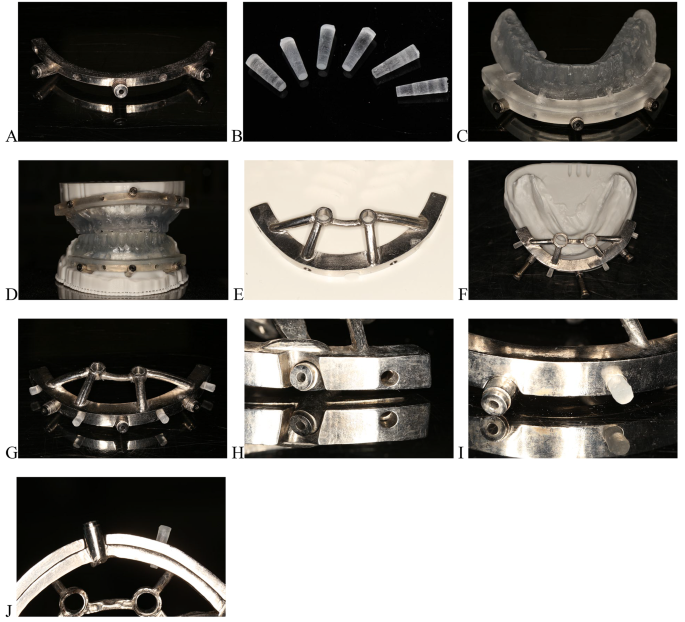
A, Mandibular base template. B, Cone-wedges. C, Mandibular 3D-printed positioning template. D, Assembled positioning template placed on the model (stackable guide 1). E, Mandibular implant placement template. F, Assembled implant placement template placed on the mandibular model (stackable guide 2). G, Assembled implant placement template. H, Insertion hole on the base template. I. J, E. F, Cones connecting the base template and implant placement templates in a horizontal direction (details of the assembled stackable guide)
-
4.
Check the fit of the 3D-printed positioning templates and the base templates intraorally before surgery. Administer local anesthesia only at fixation pin sites. Use the positioning template and silicone bite to locate the metallic retainer base templates, and fit assembly pins into the maxillary and mandible (Fig. 4A, B). Administer local anesthesia at the implant sites after removing the positioning template. Make horizontal incisions at the crest of the alveolar ridge and vertical incisions at the middle of the arch, followed by flap elevation.
Fig. 4 
Intraoral photographs of the surgery. A, Positioning of 3D-printed positioning temporary teeth. B, Placement of maxillary retention template. C, Maxillary implant placement template was inserted into the base template by cone-wedges in a horizontal direction. D, Implant placement in maxillary. E, Placement of mandibular retention templates. F, Mandibular implant placement template was inserted into retention template by cones in a horizontal direction. G, Implant placement in mandible. F, Interim implant-supported complete prosthesis in maxillary and complete denture in mandible. I, The impression was taken with polyether materials. J, Interim implant-supported complete prosthesis in the maxillary model
-
5.
Position and stabilize the metallic implant placement template on the base template using cones in a horizontal direction, and perform osteotomies following a preoperative-guided implant surgical plan (Fig. 4C). Place four dental implants (5 × 15 mm [2 in total], 4.3 × 13 mm [2 in total], Nobel Biocare Active) in the maxilla with an insertion torque of over 35 Ncm. Place the multi-unit abutments, close the wound, and take impressions with polyether materials (Fig. 4D, I).
-
6.
Fabricate a new maxillary implant-supported fixed full-arch temporary prosthesis based on the pre-operative complete denture and maxillomandibular relations (Fig. 4H, J).
-
7.
Position and stabilize the metallic implant placement template on the base template using four cone-wedges in the horizontal direction and make osteotomies following a preoperative-guided implant surgical plan (Fig. 4E, F). Place two dental implants (5 × 11.5 mm, Nobel Biocare Active) in the mandible under an insertion torque of > 35 Ncm (Fig. 4G). Finally, reline the mandible complete mandibular denture after removing the sutures.
-
8.
Verify the occlusion and finish the temporary prosthesis.




Discussion
Stackable surgical guides are popular among edentulous patients because they can avoid repeated removal of bone retainer pins [8, 13, 21,22,23]. However, retention and stability between the two elements of the stackable guide, which is separated into a base template and an upper-structure template, are crucial for surgical accuracy.
In previous reports, the anchoring mechanism was mainly classified as strut-inserted anchoring [13], snap anchoring [8, 17, 24], magnet anchoring [14,15,16], and pin-latch anchoring [18, 25]. Strut-inserted anchoring method requires high printing accuracy and the shrinkage characteristics of the printing material are also crucial. Snap anchoring method runs the risk of moving and rotating after being seated, like Locator® attachment system [26]. The magnet anchoring method leads to easy positioning attributed to the attraction force between magnets, but the strength of the attraction force affects the stability of the guides [14]. Pin-latch anchoring method can provide steady mechanical retention. The proposed technique uses a cone-wedge anchorage to connect the templates to the base template, which belongs to the pin-latch anchoring method. The cone-wedge design has several unique advantages. First, the cone-wedges were designed with a large diameter at one end and a small diameter at the other end (Fig. 3B) such that they could firmly clamp the base template and the upper-structure templates together by the force of friction. Second, it is more convenient to change the templates by inserting or removing cone-wedges of the same size into the retention holes. Third, the cone-wedges are easily positioned, even under the condition of minor misfits between the templates. However, there are fewer relevant studies on the connection types of stackable guides, and it is inconclusive which anchorage type is the most reliable.
Resin is the most commonly used material for a surgical guide, but it is easily deformed and requires a certain thickness to ensure strength [27]. The upgrade from resin to a metal 3D printing stackable guide provides better visibility of the alveolar ridge, operative space, and water cooling [13]. The proposed metal stackable guide includes three independent components: the base template which is fixed on the alveolar ridge by fixation pins; the occlusal positioning template (the upper structure 1); and the implant placement template (the upper structure 2). The upper structure templates were connected to the base template using several cone-wedges in a horizontal direction. Horizontally positioned wedges can strictly prevent the tilting of one end of the drilling template when the pressure from the drill and handpiece is applied vertically on the other end of the template. It was also found that this technique had better resistance to drill motion-caused loosening and better stabilization of the guide [28]. Therefore, this technique can accelerate operations and improve the patient experience.
The 6th International Team for Implantology Consensus Conference proceedings revealed a mean error of 1.2 mm at the entry point and 1.4 mm at the apical point, with a deviation of 3.5 degrees [25]. There was a significant difference in favor of partially edentulous cases compared with fully edentulous cases. The mean error for an entry point was 1.3 mm and that for the apex is 1.5 mm, with an angular deviation of 3.3 degrees, for fully edentulous cases [29]. Compared with other related studies, the additively manufactured, magnetically retained, and stackable resin implant surgical guide demonstrated implant angulation discrepancies ranging from 0 to 3.8 degrees, with 3D discrepancies at the coronal and apical region ranging from 0.07 to 1.73 mm and 0.07 to 1.91 mm, respectively [13]. The stackable restrictive surgical guides with a metal framework showed implant angulation discrepancies ranging from 3.19 to 9.99 degrees, and 3D discrepancies at the coronal and apical region ranged from 0.30 to 1.21 mm and 0.87 to 1.98 mm, respectively [15]. Here, the linear deviations in this technique ranged from 0.68 to 1.47 mm (mean = 0.97 mm) at the coronal implant region and from 0.78 to 2.14 mm (mean = 1.56 mm) at the apex. The angular deviations ranged from 0.98 to 4.62 degrees (mean = 2.95 degrees) (Table 1). According to a variation analysis between the virtual planning and the postplacement implant positions, the proposed technique produced fewer coronal implant deviations, and the apex and angular deviations were within the clinically acceptable range.
However, the manufacture of a metal stackable surgical guide requires high precision and accuracy. And it is more expensive than resin materials, which may pose limitations for widespread clinical applications. Therefore, further research and development in SLM technology are required to overcome these issues.
Summary
This article describes a novel cone-wedge anchored metal stackable surgical guide that aims to promote the templates’ stability and implant placement accuracy.
Data availability
The datasets used and/or analyzed during the current study are available from the corresponding author upon reasonable request.
References
Tahmaseb A, Wismeijer D, Coucke W, Derksen W. Computer technology applications in surgical implant dentistry: a systematic review. Int J Oral Maxillofac Implants. 2014;29:25–42.
Vercruyssen M, Laleman I, Jacobs R, Quirynen M. Computer-supported implant planning and guided surgery: a narrative review. Clin Oral Implants Res. 2015;26(Suppl 11):69–76.
Wismeijer D, Joda T, Flugge T, Fokaset G, Tahmaseb A, Bechelli D et al. Group 5 ITI Consensus Report: Digital technologies. Clin Oral Implants Res. 2018;29 Suppl 16:436–442. Clin Oral Implants Res 2018;29 Suppl 16:436–442.
Kernen F, Kramer J, Wanner L, Wismeijer D, Nelson K, Flügge T. A review of virtual planning software for guided implant surgery-data import and visualization, drill guide design and manufacturing. BMC Oral Health. 2020;20:1–10.
Neugebauer J, Stachulla G, Ritter L, Dreiseidler T, Mischkowski RA, Keeve E, et al. Computer-aided manufacturing technologies for guided implant placement. Expert Rev Med Devices. 2010;7:113–29.
Chackartchi T, Romanos GE, Parkanyi L, Schwarz F, Sculean A. Reducing errors in guided implant surgery to optimize treatment outcomes. Periodontol 2000. 2022;88:64–72.
Abduo J, Lau D. Effect of manufacturing technique on the accuracy of surgical guides for static computer-aided implant surgery. Int J Oral Maxillofac Implants. 2020;35:931–8.
Orgev A, Pellerito J, Polido W, Morton D, Lin WS. Bead-anchored surgical templates for static computer-assisted implant surgery: a dental technique. J Prosthodont. 2022;31:722–7.
Cushen SE, Turkyilmaz I. Impact of operator experience on the accuracy of implant placement with stereolithographic surgical templates: an in vitro study. J Prosthet Dent. 2013;109:248–54.
El Kholy K, Ebenezer S, Wittneben JG, Lazarin R, Rousson D, Buser D. Influence of implant macrodesign and insertion connection technology on the accuracy of static computer-assisted implant surgery. Clin Implant Dent Relat Res. 2019;21:1073–9.
El Kholy K, Janner SFM, Schimmel M, Buser D. The influence of guided sleeve height, drilling distance, and drilling key length on the accuracy of static computer-assisted implant surgery. Clin Implant Dent Relat Res. 2019;21:101–7.
El Kholy K, Lazarin R, Janner SFM, Faerber K, Buser R, Buser D. Influence of surgical guide support and implant site location on accuracy of static computer-assisted implant surgery. Clin Oral Implants Res. 2019;30:1067–75.
Yang JW, Liu Q, Yue ZG, Hou JX, Afrashtehfar KI. Digital workflow for full-arch immediate implant placement using a stackable surgical guide fabricated using SLM technology. J Prosthodont. 2021;30:645–50.
Costa AJM, Teixeira Neto AD, Burgoa S, Gutierrez V, Cortes ARG. Fully Digital Workflow with magnetically connected guides for full-arch Implant Rehabilitation following guided Alveolar Ridge reduction. J Prosthodont. 2020;29(3):272–6.
Garcia-Sala Bonmati F, Perez-Barquero JA, Ilzarbe Ripoll LM, Labaig Rueda C, Fernandez-Estevan L, Revilla-Leon M. An additively manufactured, magnetically retained, and stackable implant surgical guide: A dental technique. J Prosthet Dent. 2022;s0022-3913(12)00563-1.
Recena Orlando R, Duran Burgos P, Daoud El Bakhouti M, Mampel Jorge L, Kois JC, Revilla-Leon M. Two-piece magnet-retained shell manufactured by using milled and vat-polymerized methods for direct interim restorations. J Prosthet Dent 2022;s0022-3913(22)00359-6.
Baruffaldi A, Baruffaldi A, Baruffaldi M, Maiorana C, Poli PP. A suggested protocol to increase the accuracy of prosthetic phases in case of full-arch model-free fully guided computer-aided implant placement and immediate loading. Oral Maxillofac Surg. 2020;24(3):343–51.
Shah KC, Chao D, Wu BM, Jensen OT. Shape-memory retained complete arch guided implant treatment using nitinol (Smileloc) abutments. Oral Maxillofac Surg Clin North Am. 2019;31:427–35.
Moura GF, Siqueira R, Meirelles L, Maska B, Wang H-L, Mendonça G. Denture scanning technique for computer-guided implant-supported restoration treatment of edentulous patients. J Prosthet Dent. 2021;125:726–31.
Terzioğu H, Akkaya M, Ozan O. The use of a computerized tomography-based software program with a flapless surgical technique in implant dentistry: a case report. Int J Oral Maxillofac Implants. 2009;24:137–42.
Hala AH, Ahmed H. Comparative assessment of the positional accuracy of dental implants inserted using computerised stackable surgical guides made using selective laser melting and digital light processing technologies for patients with maxillary terminal dentition. Int J Oral Implantol (Berl). 2023;16(2):135–44.
Fernando GB, Jorge A, Luis IR, Carlos L-R, Lucia F-E, Marta R-L. An additively manufactured, magnetically retained, and stackable implant surgical guide: a dental technique. J Prosthet Dent. 2023;130(4):444–52.
Medhat SA, Eman T. Digital design and manufacture of a stackable implant surgical guide for immediate loading in completely edentulous full-arch cases: a dental technique. Quintessence Int. 2023;54(9):750–5.
Orentlicher G, Horowitz A, Kobren L. Computer-guided dental implant treatment of complete arch restoration of edentulous and terminal dentition patients. Oral Maxillofac Surg Clin North Am. 2019;31:399–426.
Papaspyridakos P, De Souza A, Bathija A, Kang K, Chochlidakis K. Complete digital workflow for mandibular full-arch implant rehabilitation in 3 appointments. J Prosthodont. 2021;30:548–52.
MA EL, Dayekh MA, Khalifa AK. Locator Versus Bar attachment effect on the Retention and Stability of Implant-retained Maxillary overdenture: an in Vitro Study. J Prosthodont. 2019;28(2):e627–36.
Piedra-Cascon W, Mostafavi D, Ruiz-de-Gopegui J, Perez-Pevida E, Robles-Cantero D, Revilla-Leon M. Fabricating a dual-material, vat-polymerized, additively manufactured static implant surgical guide: a dental technique. J Prosthet Dent. 2022;128(3):233–8.
Hang-Nga M, Du-Hyeong L. Effects of supporting conditions and anchor microscrew on the stabilization of the implant guide template during the drilling process: an in vitro study. J Prosthet Dent. 2020;124(6):727.e1-727.e8.
Tahmaseb A, Wu V, Wismeijer D, Coucke W, Evans C. The accuracy of static computer-aided implant surgery: a systematic review and meta-analysis. Clin Oral Implants Res. 2018;29(Suppl 16):416–35.
Acknowledgements
We thank technician Yuetao Hao for supporting our study.
Funding
This project was supported by the United Fund of Innovative and Developmental Science Foundation of Hubei Province (2022CFD005) and NSFC (82071090).
Author information
Authors and Affiliations
Contributions
Xueying Bai: Project administration, Roles/Writing - original draft.
Tao Wu: Formal analysis, Methodology, Roles/Writing - original draft, Supervision.
Yuxi Zhu: Data curation, Project administration,
Chengyu Yang: Investigation, Software.
Tiange Cheng: Visualization, Software.
Yi Liu: Funding acquisition, Validation.
Yi Zhou: Conceptualization, Funding acquisition, Writing - review &editing.
Corresponding author
Ethics declarations
Ethics approval and consent to participate
All methods were carried out in accordance with relevant guidelines and regulations. All experimental protocols were approved by the Independent Ethics Committee of School and Hospital of Stomatology, Wuhan University (2023B40).
Consent for publication
Not applicable.
Competing interests
There is no conflict of interest affecting any of the authors of this work.
Additional information
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Electronic supplementary material
Below is the link to the electronic supplementary material.
Rights and permissions
Open Access This article is licensed under a Creative Commons Attribution 4.0 International License, which permits use, sharing, adaptation, distribution and reproduction in any medium or format, as long as you give appropriate credit to the original author(s) and the source, provide a link to the Creative Commons licence, and indicate if changes were made. The images or other third party material in this article are included in the article’s Creative Commons licence, unless indicated otherwise in a credit line to the material. If material is not included in the article’s Creative Commons licence and your intended use is not permitted by statutory regulation or exceeds the permitted use, you will need to obtain permission directly from the copyright holder. To view a copy of this licence, visit http://creativecommons.org/licenses/by/4.0/.
About this article

Cite this article
Bai, X., Wu, T., Zhu, Y. et al. Cone-wedge anchored surgical templates for stackable metal guide: a novel technique. Int J Implant Dent 10, 27 (2024). https://doi.org/10.1186/s40729-024-00539-w
Received:
Accepted:
Published:
DOI: https://doi.org/10.1186/s40729-024-00539-w